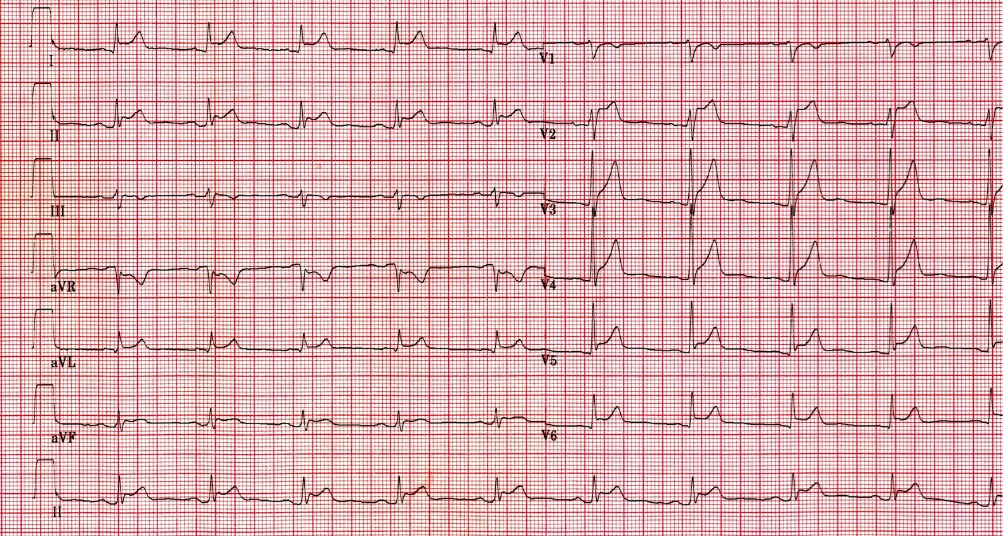
A 43-year-old male with recent upper respiratory illness presents to the ED with 3 days of substernal chest pain worse with deep inspiration. Electrocardiogram is shown. Laboratory results reveal a leukocytosis and a normal troponin level. What is the best treatment for this disease?
B) NSAIDs and colchicine is correct
A. Heparin – INCORRECT
This patient presentation and ECG are consistent with acute pericarditis, not acute coronary syndrome or pulmonary embolism.
B. NSAIDs and colchicine – CORRECT
Pericarditis is defined as inflammation of the outer layer of the heart (the pericardium). The majority of cases are idiopathic, but other causes include infections, connective tissue disease, uremia, malignancy and Dressler’s syndrome. Symptoms include substernal chest pain that is exacerbated by deep inspiration and relieved by leaning forward, fatigue, and intermittent fever. The hallmark of pericarditis is a pericardial friction rub. ECG classically shows diffuse ST elevations as well as PR depressions. Diagnosis is made by electrocardiogram (ECG) in conjunction with chest radiography, echocardiogram and laboratory studies. Echocardiogram is used to rule-out pericardial effusion and a chest x-ray may reveal changes related to an underlying pericardial effusion, such as a boot-shaped heart. Approach to treatment includes addressing the underlying cause, NSAIDs or Aspirin, narcotics for pain, and steroids in patients with chronic or recurrent pericarditis, or in those patients who cannot tolerate NSAIDs.
For patients with acute first-episode idiopathic or viral pericarditis, colchicine is recommended as adjunctive therapy to NSAIDs or aspirin, as colchicine has been shown to reduce recurrence rates and decreases symptom severity.
C. Steroids – INCORRECT
Glucocorticoids are generally reserved for pericarditis that is refractory to NSAID/aspirin and colchicine treatment.
D. Tenecteplase – INCORRECT
This patient presentation and ECG is consistent with acute pericarditis, not ST-elevation myocardial infarction or pulmonary embolism.


By the way, do you read JournalFeed?
Through the joint providership of Hippo Education and JournalFeed, you can now get up to 27 AMA PRA Category 1 Credits™ for reading JournalFeed.
Yes, please! Learn more about JournalFeed CME